COPD Right Care update November 2021

November 17th is World COPD Day with a focus on maintaining healthy lungs. Primary care has an essential role to help people maintain the best lung health in order to avoid COPD or to help them live a better life with COPD. In this edition we start with our framework describing the key components of COPD Right Care that reveals the importance of strengthening local primary and community care systems.
We then highlight:
- Considerations for treating tobacco dependency, following the WHO Essential Medicines List 2021 update
- A report on the development of two new IPCRG tools to help start different conversations about safe, personalised COPD care, thanks to an educational grant from Boehringer Ingelheim.
COPD treatment at system and individual level is often characterised by overuse (e.g. oral steroids and antibiotics), misuse (e.g. oxygen) and underuse (e.g. smoking cessation, immunisation and pulmonary rehabilitation) and these elements together provide poor value healthcare.
We use the concept of Right Care as explained by the Lancet series 2017: “the shared challenge is ensuring the right care is received by the right patients, in the right setting, at the right time, at the right cost.” We would add “in the right way”.
As with the Asthma Right Care programme, our starting point is that education alone doesn’t solve variation and what is required is exploration of other factors in health systems such as different goals that drive different behaviours. The aspect that IPCRG believes it can impact most is the behaviour of those responsible for delivering the care.
Clinically effective and cost-effective COPD care consists of a correct, well communicated diagnosis that takes account of multimorbidity and therapy that includes multiple interventions to address personal need. Any health system or health professional will need to consider the range of interventions available for COPD and then consider their relative value to the person living with COPD after understanding their personal circumstances, goals and choices.
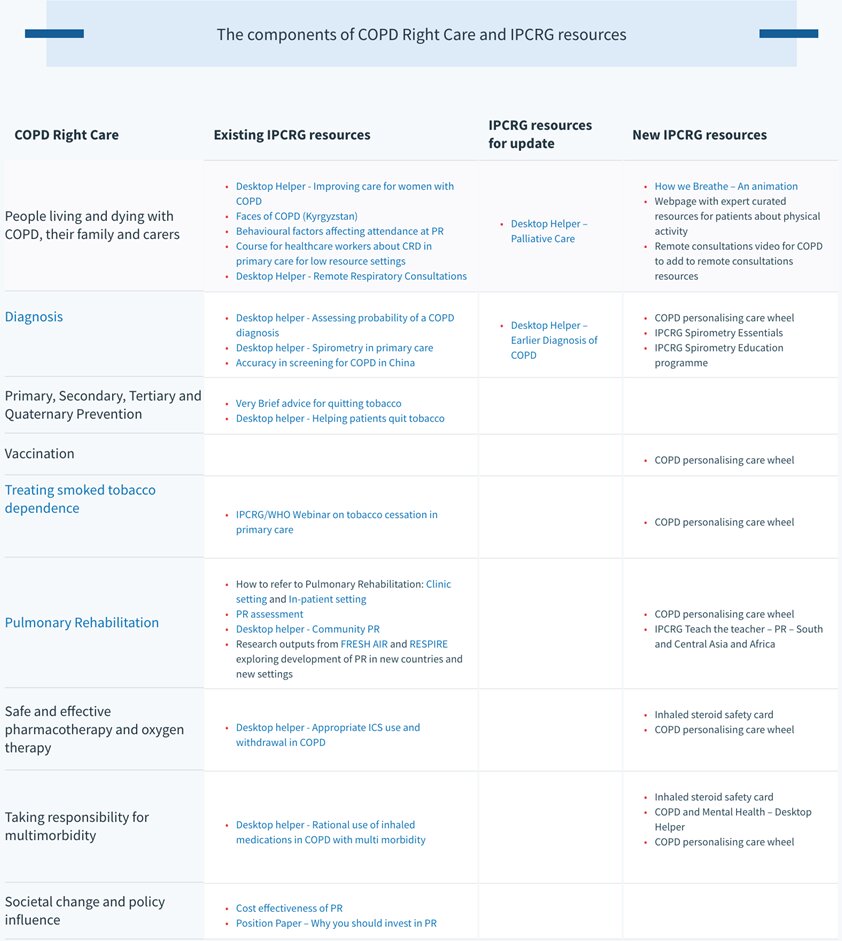
The table below highlights that we can be positive about the public health measures, diagnostic options and treatments that exist for preventing, diagnosing and treating COPD, but it should also make us question as individual practitioners or health system coordinators whether we seek to provide this offer or whether we are limiting ourselves to a narrow field of options or a one size fits all model?
In COPD Right Care we will work with members to start a movement in countries that moves people to thinking about COPD care in a personalised and holistic way and then signpost to resources which will then feel relevant and continue to develop resources where we identify a need.
Update on Treating Tobacco Dependency
The World COPD Day theme of healthy lungs focuses on causation of COPD and in primary care we can advise and support people about risks related to their occupation and the air they breathe indoors and outdoors. Adjusting their risks following any practitioner advice then depends on a complex mix of societal, community, family and individual actions. However, the primary care practitioner can intervene in many ways with evidence-based interventions for managing the risk of tobacco smoking.
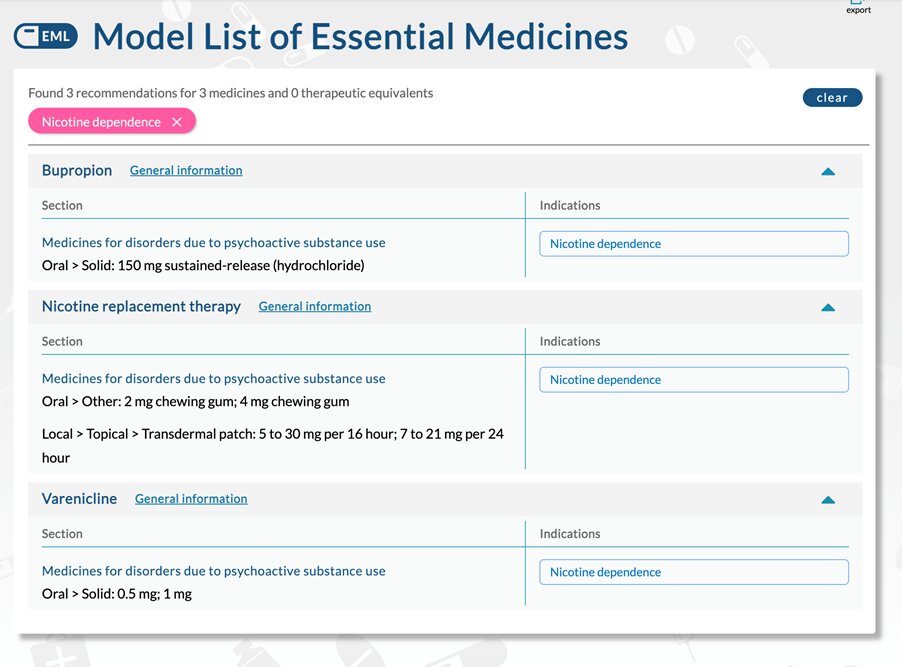
The World Health Organisation, 22nd Essential Medicines List was released in October 2021 and now includes two new medicines in addition to Nicotine Replacement Therapy as essential for national formularies:

Primary care can use this information at system level to lobby and encourage the uptake of the WHO classification to ensure these medicines are available on national formularies. We know that treating tobacco dependence can be a long-term intervention before a final persisting sustained quit is achieved and primary care practitioners need a range of behavioural and pharmacotherapy tools as they move towards this goal. Moving to three therapies that enables dual and short and long acting versions of therapy enhances the treatment options we can give.
In recent months the news of supply problems of varenicline due to an investigation into potentially harmful, N-nitroso-varenicline levels further clarifies the need to have multiple therapy options. IPCRG was part of a submission from clinicians, public health specialists, academics, and researchers committed to the WHO Framework Convention on Tobacco Control that requested Cytisine to be included on this list due to its efficacy, cost-effectiveness and acceptability to many groups of tobacco users. Unfortunately, it was not included but we know our member countries would benefit from this option and will continue to support inclusion on national formularies.
The addition of these medicines aligns with another WHO campaign in 2021/22. The focus of the 2021 year long World No Tobacco Day (WNTD) campaign is quitting tobacco. WHO has called for bold and transformative steps which are needed to encourage and support tobacco users worldwide to quit tobacco use. WHO also aims to ensure at least 100 million tobacco users are empowered with necessary knowledge and have access to tools to make a quit attempt. In June 2021 IPCRG partnered with WHO to produce a webinar discussing how primary care clinicians can role model and lead this change. You can see videos of all the presentations here and our practical tobacco treatment guides and advice here.
Development and testing of two novel tools to start new conversations and challenge the status quo in 2021
Key to the success of the Asthma Right Care project was the creation and development of tools that would enable behaviour-changing conversations between health professionals and between health professionals and patients. The main tool arising from the thinking and discussions of our multi-country and multi-professional delivery team resulted in development and then country adaptations of the tool we called the SABA Slide Rule.
For COPD a team of experts in primary care COPD are coming together to build and test new tools that will generate new discussions and changes in behaviour.
We will develop two prototype concepts with two clinicians from each pilot country – Brazil ( GEPRAPS), Portugal (GRESP), Spain (GRAP), USA ( COPD Foundation), a patient expert from the US COPD Foundation and a community pharmacist from the UK. Our four pilot countries will then test these products with colleagues and patients.
We look forward to sharing the results with you in early 2022.
Noel Baxter
Joint CEO